The effectiveness of portable heat patch in protecting the health of military personnel operating in cold conditions in Northern Vietnam
Main Article Content
Abstract
This study provides a scientific basis for applying portable heat patches as auxiliary equipment to support military personnel during extreme cold weather in Northern Vietnam. An experimental survey was conducted with 50 volunteer soldiers, divided into a control group (NC) and an experimental group (TN), with no significant baseline differences in physiological indices (p > 0.05). Survival indicators (core temperature (Tcore), finger temperature (Tfinger), heart rate, blood pressure), subjective cold perception, and the heat retention capacity of the patch were monitored. Statistical methods were used to compare group differences and Pearson correlation analysis was conducted to examine the relationships between variables. The heat patch effectively supported thermoregulation, with Tcore in the TN group maintained 0.2–0.5°C higher than in the NC group, and Tfinger increased by up to 2°C, indicating improved peripheral circulation. The patch also reduced cold-induced increases in heart rate and enhanced overall thermal comfort (p < 0.05). Its temperature remained stable within the safe range of 38–43°C for up to 12 hours. Strong correlations were observed between patch temperature and cold sensation scores (r = –0.620, p < 0.01), along with moderate correlations with Tcore (r = 0.350, p < 0.01) and Tfinger (r = 0.318, p < 0.01), confirming its warming effectiveness in cold environments. Overall, the portable heat patch represents a practical, rapid-response warming solution suitable for military personnel facing sudden severe cold during winter operations in Northern Vietnam
Keywords
portable heat pad, military health, cold conditions, body temperature, Northern Vietnam
Article Details

This work is licensed under a Creative Commons Attribution 4.0 International License.
- Highlights:
The heat patch maintained core temperature and improved peripheral circulation under cold exposure (p < 0.05).
Cold-induced cardiac stress was reduced, and thermal comfort was significantly enhanced (p < 0.05).
The patch provided stable and safe heating within 38–43°C for up to 12 hours.
Offers a flexible, safe, and effective warming solution for military personnel in cold environments.
1. INTRODUCTION
Cold environments pose a significant threat to human health and performance during prolonged outdoor activities, especially in military operations. Cold stress can substantially impair physical performance, cause thermal discomfort, and increase the risk of local cold injuries (e.g., frostbite) as well as systemic hypothermia [1, 2]. Despite advancements in protective clothing and military gear for cold weather, cold-related injuries remain a major concern when individuals are exposed to low ambient temperatures. Military personnel are particularly vulnerable due to extended outdoor exposure during training and missions. A report recorded over 2,700 cold-weather-related injuries in the United States Armed Forces between 2012 and 2017 [3]. Field studies in Canada reported frostbite incidence rates as high as 21% during military training under freezing conditions [4, 5]. During World War I, there were 115,000 cold injuries reported in just four months [6].
Notably, skin temperature in extremities can drop sharply even when core body temperature is maintained, leading to a 23–28% decline in finger motor performance [7]. Epidemiological data show increased risks of hypothermia, frostbite, hospitalization, and mortality when temperatures drop below critical thresholds, such as −15°C to −29°C [8]. For each 1°C decrease below a certain threshold, mortality increases by 3.44% and hospitalization by 0.78%, especially among the elderly and those with cardiovascular or respiratory conditions [9, 10]. Prolonged cold exposure can reduce muscle strength by approximately 4%, although cognitive performance is less affected [7]. Survival in cold environments depends mainly on ambient temperature and the insulating properties of clothing, whereas the contribution of body heat generation is relatively minor [11].
In Northern Vietnam, a tropical monsoon region with relatively mild winters, the average winter temperatures in mountainous areas typically range from 13 to 15°C. However, with climate change, recent years have seen increasingly extreme weather events, with temperatures occasionally dropping below 0°C, especially in high-altitude areas like Sa Pa and Mau Son, where frost (a rare phenomenon in Vietnam) has been recorded [12]. Sudden cold spells in mountainous regions can render conventional cold-weather responses inadequate, necessitating immediate supplementary measures. In this context, compact, portable, and cost-effective heating solutions are critically needed for military operations.
Recently, chemical heat patches have become popular as a supplemental heat source. These patches consist of a mixture of heat-generating materials enclosed in an air- and moisture-permeable inner pouch [13]. Heat is generated via an exothermic reaction when the inner pouch is removed from its packaging. These devices provide localized warmth and can extend operational time in cold environments, especially for vulnerable areas like the hands, feet, and lower back. However, their performance in military field conditions, particularly in the mountainous climate of Northern Vietnam, has not been thoroughly investigated.
Therefore, the aim of this study is to evaluate the physiological and functional effectiveness of portable chemical heat patches in supporting thermoregulation and operational performance among military personnel in cold environments in Northern Vietnam. Specifically, the study aims to: (1) assess key survival indicators under cold stress; (2) evaluate users’ subjective cold perception; and (3) determine the heat retention efficiency and safety of the patch. The findings will assess the feasibility and practical value of heat patches as an auxiliary protective measure during unexpected cold weather events in the field.
2. MATERIALS AND METHODS
2.1. Portable heat patch
The portable heat patch was developed and manufactured by the Joint Vietnam-Russia Tropical Science and Technology Research Center. The patch consists of an air-permeable layer, a heat-generating layer, and an adhesive layer. An air-permeable layer is made of PP non-woven material with an air permeability of 150–300 mm/s to ensure adequate oxygen exposure to the reactive mixture and to regulate the heating rate; meanwhile, the medical-grade acrylic adhesive layer provides an adhesion strength of 13–17 N, allowing the patch to remain securely attached to clothing for up to 10 hours. The heat-generating mixture was optimized to ensure both safety and thermal efficiency. Specifically, it consisted of 33% iron powder, 14% activated carbon, and other components such as active salts, minerals, and water. The product is rectangular in shape, measuring 10 × 13 cm and weighing 32 grams. When heat patch was activated, typically by tearing the packaging or exposing it to air, these components react with each other to generate heat through the oxidation of iron powder [14, 15]. The core principle of the heat patch is an exothermic reaction based on the redox process of metallic iron, following the reaction: 4Fe + 3O₂ → 2Fe₂O₃. Iron powder acts as the primary heat-generating agent, as its oxidation is a highly exothermic reaction [13]. The patch can be directly applied to the area requiring warmth, and the reaction begins automatically upon air exposure. This process provides consistent and safe heat output, effectively supporting thermal maintenance in low-temperature conditions without the need for electricity or additional equipment.
2.2. Experimental design
The study was conducted at three border guard stations in Lang Son Province, Vietnam, under ambient temperature conditions ranging from 2.8 to 8.2°C, wind speeds of 15–21 km/h and relative humidity between 83.2% and 86.2%. Inclusion criteria required participants to be male soldiers aged 20 - 50, free from acute illness, presenting normal baseline physiological indicators, and voluntarily agreeing to participate. Exclusion criteria included any history of cardiovascular or respiratory disease, skin allergies, fever, infection, musculoskeletal injury, the use of medications affecting thermoregulation, or any inability or refusal to complete the trial. A total of 50 active-duty male soldiers in stable health were recruited and then clearly divided into two groups, with 20 participants assigned to the control group (NC) and 30 participants assigned to the experimental group (TN), following predefined inclusion and exclusion criteria. There were no statistically significant differences in baseline survival indicators between the groups (p > 0.05, Table 1). The control group (n = 20) did not use the portable heat patch and wore only the standard winter field uniform of the Vietnam People’s Army. The experimental group (n = 30) used the portable heat patches in addition to the standard uniform, applying them at three locations: the chest, lower back, and front of the thighs (Figure 1). Both groups followed an identical daily program of physical activities and military training, including marching, weapon assembly/disassembly, simulated first aid, tent setup, and continuous outdoor operations from 6:00 h to 18:00 h. Data collection was carried out every four hours at 6:00 h, 10:00 h, 14:00 h, and 18:00 h each day. Skin safety was monitored according to ISO 10993-23, focusing specifically on skin irritation and sensitization, and any participant showing abnormal symptoms was immediately withdrawn from the trial.

Figure 1. Field testing of the heat patch on military personnel
2.3. Methods for determining research indicators
2.3.1. Measurement of vital signs
Core body temperature (Tcore) was measured using the non-invasive iThermonitor WT705 temperature sensor (Wexin Technology Co., Ltd., China), which was attached under the left armpit and wirelessly connected to a handheld data recorder. This device allowed for continuous monitoring of body temperature throughout the day with an accuracy of ±0.1°C. Data were extracted daily and stored in spreadsheet format.
Skin temperature at the index finger of the dominant hand (Tfinger) was measured using the Fluke 62 MAX handheld infrared thermometer (Fluke Corporation, USA), with an accuracy of ±1.0°C and a measurement range from −30°C to 500°C. Each measurement was performed three consecutive times at a fixed distance of 3–5 cm, and the average value was recorded.
Table 1. Baseline differences in vital signs between experimental groups
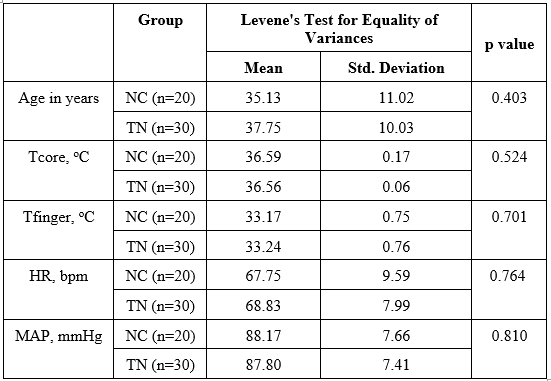
Heart rate (bpm) and blood pressure (mmHg) were measured using the Omron HEM-7120 automatic digital blood pressure monitor (Omron Healthcare, Japan). Measurements were taken while the subject was seated at rest, after at least 10 minutes of no physical activity. Each subject underwent two measurements; if the difference between them exceeded 10 units, a third measurement was taken, and the average of the two closest values was used.
The mean arterial pressure (MAP) was calculated using the following formula:

Where: MAP is the mean arterial pressure (mmHg); SBP (Systolic Blood Pressure) refers to the systolic pressure (maximum blood pressure, mmHg); and DBP (Diastolic Blood Pressure) refers to the diastolic pressure (minimum blood pressure, mmHg).
2.3.2. Assessment of subjective cold sensation score
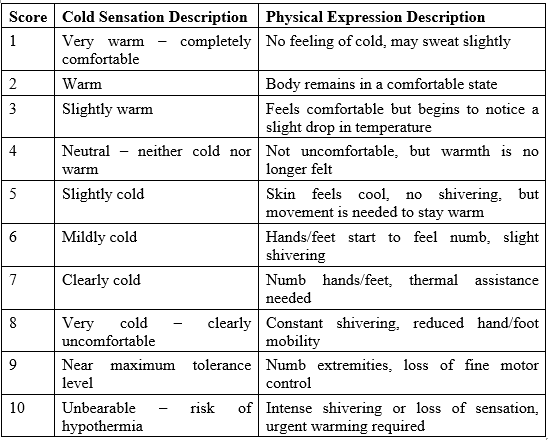
Cold Sensation Score (CSS) was evaluated using a 10-point scale, with clearly defined descriptors for each level (Table 2). Each soldier was instructed to self-record their cold sensation score at predefined time points throughout the day.
Table 2. Subjective cold sensation rating scale
2.3.3. Measuring the surface temperature of the heat patch
The heat-retention capacity of the patch was determined by measuring its surface temperature using a Fluke 62 MAX infrared thermometer (USA) at specific times: 6:00 h (10 minutes after application), 10:00 h, 14:00 h, and 18:00 h. The patches were applied to the chest, lower back, and front thigh, over a layer of protective clothing. Each measurement was performed three consecutive times at a distance of 5–8 cm, and the average value was recorded to minimize error. The surface temperature value of the heat patch represents the average temperature measured across the three positions. The recorded surface temperatures reflect the heat generation and stability of the patch under outdoor cold field conditions.
2.4. Data analysis method
Data were collected and organized using Microsoft Excel 365 (Windows version), while all advanced statistical analyses (Independent Samples T-Test and Pearson correlation analysis) were performed using SPSS software (version 20, Windows). The Independent Samples T-Test was applied to assess differences between the two experimental groups, with statistical significance set at p < 0.05. The Pearson correlation coefficient (r) was used to determine the strength and direction of the linear relationship between two variables, with values ranging from -1 to 1. An r value of 1 represents a perfect positive linear relationship, while an r value of -1 indicates a perfect negative linear relationship. An r value of 0 suggests no linear correlation. The correlation strength was classified as follows: very weak (0.00–0.10), weak (0.10–0.39), moderate (0.40–0.69), strong (0.70–0.89), and very strong (0.90–1.00) [16]. The statistical significance of the correlation was determined by the p-value, with p < 0.05 indicating a significant correlation.
3. RESULTS
3.1. Differences in vital signs
Exposure to cold conditions can negatively affect vital signs (Figure 2). The use of heat patches demonstrated positive effects. During the experiment, the TN group maintained a higher and more stable core body temperature, while the NC group showed several values below 36.0°C, indicating mild hypothermia. This difference persisted throughout the day, particularly at 10:00 h and 14:00 h, where the TN group consistently had significantly higher core temperatures compared to NC (p < 0.05). The heat patches improved core temperature maintenance by supplying heat to central body areas (chest, abdomen, lower back), aiding thermoregulation. This finding is consistent with Marrao et al. (2005), who reported that maintaining core warmth supports normal function in prolonged cold exposure [7].
The study results indicated that the TN group also had significantly higher fingertip skin temperatures compared to the NC group (p < 0.05). The differences were especially marked at 10:00 h and 14:00 h, indicating better peripheral circulation in the TN group. Many values in the NC group dropped below 30°C, a threshold associated with reduced manual dexterity and increased frostbite risk. Peripheral skin temperature was better maintained due to reduced peripheral vasoconstriction, a result of effective core warming. This mechanism is supported by the CoWEDA physiological model, which shows that warming the body core enhances peripheral blood flow and reduces cold injury risk [17]. Additionally, Daanen (2003) affirmed that maintaining safe peripheral skin temperature helps prevent cold-induced tissue damage [18].
Heart rate differences between the TN and NC groups highlighted the cardiovascular impact of active warming. Between 10:00 h and 14:00 h, the TN group had significantly lower heart rates than the NC group (p < 0.05). This reflects a physiological adaptation: without external heat, the body must increase sympathetic nervous activity to trigger vasoconstriction and generate endogenous heat, leading to elevated heart rate [2, 19]. Conversely, the TN group benefited from exogenous heat input, reducing cold stress response, stabilizing circulation, and eliminating the need for compensatory heart rate elevation.
Mean arterial pressure remained within the normal range (approximately 85–88 mmHg) for both groups. However, the TN group exhibited slightly lower MAP values at 10:00 h, 14:00 h, and 18:00 h, indicating reduced peripheral vasoconstriction (a beneficial effect), although the differences were not statistically significant (p > 0.05). Ikäheimo et al. (2020) emphasized the influence of ambient temperature on blood pressure and cardiovascular risk among outdoor workers [10]. Other studies have shown that reducing vasoconstriction through active warming can lessen cardiovascular strain in cold environments [20]. These findings demonstrate that the heat patch not only supports core temperature maintenance but also optimizes cardiovascular responses, thereby reducing physiological burden in extreme cold conditions.
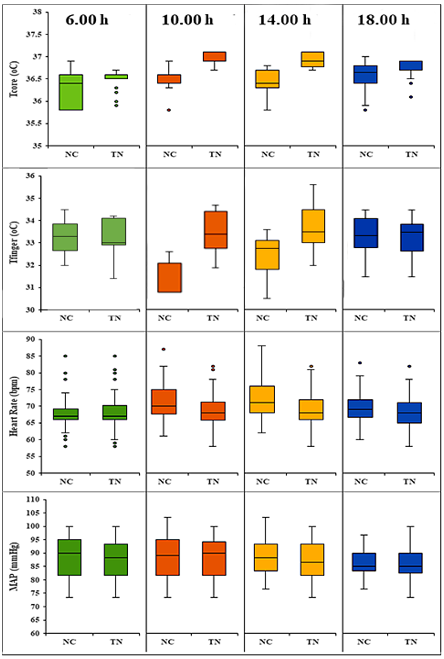
Figure 2. Vital sign results of the two surveyed groups (NC: control group; TN: experimental group)
3.2. Subjective sensation evaluation
Survey results on cold perception levels showed that the group using the heat patch (TN) consistently reported significantly lower cold sensations than the non-using group (NC) at all time points during the day. At the lowest ambient temperature, 6:00 h, the NC group recorded an average score of 6.16 ± 0.42, corresponding to a “mild cold” sensation with symptoms such as numb hands/feet and slight shivering. In contrast, the TN group reported a much lower score of 3.80 ± 0.49, indicating a “neutral – neither cold nor warm” sensation, reflecting noticeable comfort even at the coldest time of day. By 10:00 AM, the difference persisted, with the NC group averaging 4.76 ± 0.43 (slightly cold), while the TN group scored 2.38 ± 0.49 (warm), confirming the patch’s ability to maintain comfort. Similarly, at 14:00 h, the TN group continued to report lower cold sensation (3.16 ± 0.51) compared to the NC group (4.28 ± 0.45). At 18:00 h, the TN group reported an increased sensation score of 5.28 ± 0.81 (slightly cold), indicating a reduction in patch warming efficiency over time, but still lower than the NC group’s score of 6.06 ± 0.24. These results clearly show that the heat patch significantly improves thermal comfort by reducing cold sensation from “mild cold” or “slightly cold” to “neutral” or “warm,” and helps alleviate cold-related physiological symptoms such as shivering and numbness in extremities. This supports the practical utility of the patch in promoting thermoregulation and comfort in cold environments. These findings are consistent with previous studies indicating that exogenous heat sources improve thermal perception and reduce discomfort associated with cold exposure [21]. Bauman et al. (1998) also reported that using warming devices with a fixed surface temperature significantly enhances thermal sensation and user comfort in cold environments [22]. Additionally, the heat patch did not cause any discomfort or overheating sensations during use.
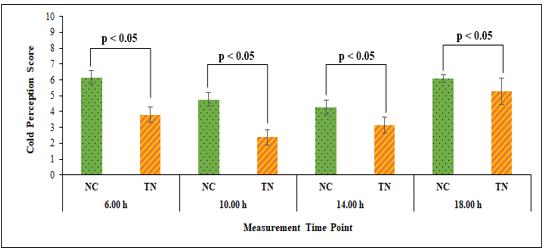
Figure 3. Subjective cold sensation survey results (NC: control group; TN: experimental group)
3.3. Heat retention efficiency and safety of the heat patch
Throughout the testing period from 6:00 h to 18:00 h, the surface temperature of the heat patch (Thp) showed a gradual decline, accurately reflecting the heat generation mechanism of iron powder upon exposure to air. Specifically, at 6:00 h, the heat patch reached its peak average temperature of 42.98 ± 0.58°C and remained stable at 42.90 ± 0.22°C up to 10:00 h, indicating that the oxidation reaction was highly active and efficient during the initial usage phase. This observation aligns with findings from Klarzak et al. (2018), which demonstrated that the oxidation of iron powder can generate temperatures up to 45°C before gradually declining [13]. After 10:00 h, the patch temperature began to decrease significantly, reaching 40.85 ± 0.79°C at 14:00 h and dropping to its lowest point of 38.96 ± 0.73°C by 18:00 h. Despite the downward trend, the temperature consistently remained within the safe range of 38–43°C, which is considered safe for direct skin contact and conforms to ASTM C1055-20 standards for burn thresholds [23]. Langer et al. (2017) reported that skin exposure to temperatures below 44°C is generally safe for prolonged contact [24]. These results indicate that the heat patch not only demonstrates a strong heat-generating effect but also maintains effective thermal retention for up to 12 hours. This makes it suitable for use in cold environments to help prevent hypothermia.
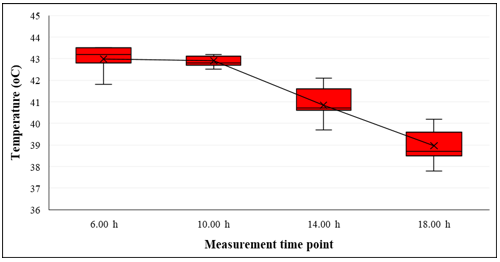
Figure 4. Surface temperature of the heat patch during the testing period
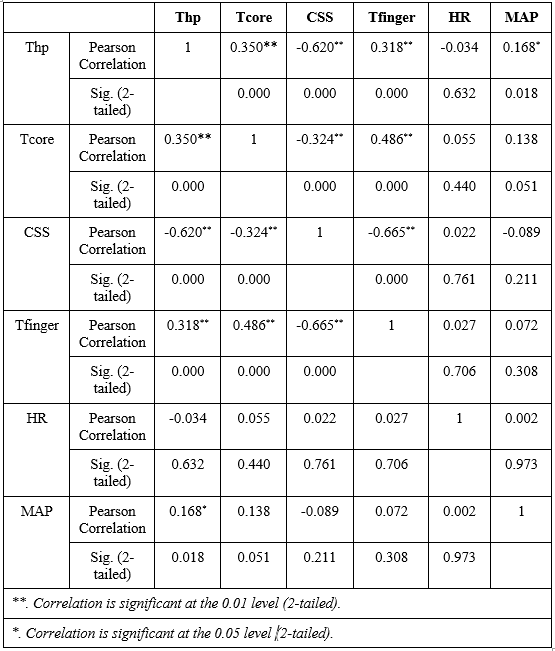
The results of the Pearson correlation analysis showed that Thp had a strong negative correlation with CSS (r = -0.620, p < 0.01), indicating that as the surface temperature of the patch increased, users experienced a significant decrease in cold sensation. Conversely, Thp was positively correlated with Tcore (r = 0.350, p < 0.01) and Tfinger (r = 0.318, p < 0.01), suggesting that the heat generated by the patch contributed to maintaining both core and peripheral body temperatures, thereby limiting vasoconstriction and heat loss in the extremities. In contrast, Thp showed no significant correlation with heart rate (p > 0.05), indicating that use of the heat patch did not noticeably affect heart rate. This implies that exogenous heat helps reduce cold stress and stabilize cardiovascular responses without overstimulation. Additionally, Thp showed a slight positive correlation with MAP (r = 0.168, p < 0.05), possibly due to localized peripheral vasodilation without significantly impacting systemic blood pressure. Importantly, no participants reported any signs of skin irritation or sensitization during or after the trial, further confirming that the heat patch is safe to use.
Table 3. Pearson correlation analysis results
4. DISCUSSION
Vietnam is a tropical monsoon country where winters are generally mild, with cold periods that are short, irregular, and heavily influenced by monsoon patterns. In contrast, countries such as those in Northern Europe, North America, or Northeast Asia routinely face prolonged freezing weather, snowfall, strong winds, and sustained subzero temperatures, requiring their military forces to be equipped with thick multilayered clothing, insulated boots, electrically heated garments, and high-capacity thermal gear. However, recent climate changes have brought sudden cold waves, with temperatures occasionally dropping below 0°C, posing serious health risks, especially for northern Vietnam border patrol forces who must operate outdoors for extended periods. In this context, enhancing cold-weather protection poses challenges due to limited budgets and the infrequency of extreme cold events, which makes it inefficient to permanently issue bulky cold-weather gear. The use of portable chemical heat patches presents a practical interim solution, compact, low-cost, and capable of rapid deployment in response to sudden temperature drops. The findings of this study clearly demonstrate the effectiveness of these heat patches in maintaining thermal balance for over 8 hours, significantly reducing cold sensation and helping to stabilize key physiological parameters such as core and peripheral temperatures. The heat patch works by delivering direct warmth to central body regions, helping maintain a stable core temperature and reducing cold-induced vasoconstriction, thereby improving peripheral circulation and maintaining warmer skin. When the core is warmed, sympathetic activation decreases, limiting heart-rate elevation and reducing the need for endogenous heat production, which stabilizes hemodynamics and lowers physiological strain in cold environments [2, 19]. These results are especially important for field units that operate in remote or mountainous areas where other heating equipment may not be feasible. Moreover, the strong negative correlation between patch temperature and subjective cold sensation, and the positive correlation with both Tcore and Tfinger, confirm that the heat patch directly contributes to improving thermal comfort and physiological stability in cold conditions. Importantly, the patch did not significantly affect heart rate or mean arterial pressure, reinforcing its safety for extended use without causing cardiovascular strain. These findings are largely consistent with previous research. For example, Knecht et al. (2016) reported that wearable thermal-management systems significantly improve thermal comfort [25]. Likewise, Irzmańska et al. (2020) indicated that iron-powder-based warming devices can enhance hand dexterity and maintain thermal comfort [15]. In addition, the use of skin-applied thermal patches can promote blood circulation and reduce pain [26]. Taken together, the portable chemical heat patch offers a viable, efficient, and scalable solution for military personnel operating in unpredictable and harsh cold environments, especially in countries like Vietnam where extreme winter weather is episodic rather than constant. Integrating such devices into cold-weather readiness protocols could enhance operational endurance, reduce cold-related injuries, and improve overall troop morale in the field.
Although the study provides promising evidence regarding the applicability and safety of the heat patch, several potential limitations should be acknowledged. Because the study was conducted under natural field conditions, ambient temperature, wind speed, and humidity fluctuated throughout the observation period, limiting environmental control and potentially influencing thermal and cardiovascular responses. The participant cohort consisted exclusively of healthy male soldiers aged 20–50, which restricts external validity and limits the generalizability of the findings to other demographic groups. Moreover, the study evaluated physiological responses only within a 24-hour period, without assessing longer-term or cumulative effects of repeated heat-patch use or the possibility of delayed skin irritation or sensitization. The results may also have been influenced by uncontrolled confounders, including inter-individual differences in body fat percentage, habitual physical activity levels, and diet-related thermogenesis, all of which affect cold tolerance and metabolic heat production. Additionally, the cold sensation score relies on subjective perception, which may introduce variability despite standardized instructions. Overall, future research conducted under controlled climatic conditions, with more diverse participant populations and longer follow-up durations, will be necessary to validate and extend these findings.
5. CONCLUSION
This study demonstrates that the use of heat patches under cold conditions has a significant positive effect on improving vital signs, enhancing thermal sensation, and ensuring physiological safety for users. Specifically, TN group maintained higher core body and peripheral skin temperatures compared to NC group, thereby reducing the risk of hypothermia and frostbite. The TN group also exhibited lower heart rates, reflecting more stable circulation and a reduced cold stress response, although MAP did not show a statistically significant difference. Furthermore, cold sensation was significantly improved in the TN group, contributing to greater comfort and reducing cold-related symptoms such as shivering and extremity numbness. In terms of heat retention, the patch maintained a safe and stable surface temperature within the range of 38–43°C for up to 12 hours, aligning with skin contact safety standards and posing no risk of burns. The correlations between patch surface temperature and physiological indicators, such as core temperature, peripheral skin temperature, and cold sensation, further confirm the product's safety and effectiveness. Overall, the portable chemical heat patch is a practical and effective method for supporting thermoregulation, reducing physiological strain, and enhancing comfort in cold environments. Future studies may focus on optimizing heat patch formulation, evaluating long-term field performance across different climatic regions, and integrating heat patches into broader cold-weather protection strategies for military and civilian applications.
Acknowledgments: This study was financially supported by the Joint Vietnam - Russia Tropical Science and Technology Research Center in the project with the approval decision number 3665/QĐ-TTNĐVN dated 02 October 2023.
Statement on the use of Generative AI: The authors declare that AI tools were used only for language editing/formatting, and not for generating scientific content. All data, analyses, and interpretations were performed and verified by the authors, who take full responsibility for the manuscript.
Author contributions: Nguyen Thi Thu Thuy: conceptualization, methodology, writing; Nguyen Van Thanh: review and editing, data analysis; Bui Dinh Khai: methodology, data collection; Dao Nguyen Manh: supervision; Quach Thi Quynh: data collection, supervision; Pham Thi Phuong Lien: data collection; Vu Thi Loan: review and editing.
Conflict of interest statement: The authors declare that there are no conflictsof interest related to this article.
References
2. H. Rintamäki, Human responses to cold, Alaska Med, Vol. 49, No. 2, pp. 29–31, 2007.
3. F. L. O’Donnell, S. Stahlman and A. A. Oetting, Update: Cold weather injuries, active and reserve components, U.S. Armed Forces, July 2012–June 2017, MSMR, Vol. 24, No. 10, pp. 12–21, 2017.
4. W. Sullivan-Kwantes, P. Dhillon, L. Goodman and J. J. Knapik, Medical encounters during a joint Canadian/U.S. exercise in the high Arctic (Exercise Arctic Ram), Military Medicine, Vol. 182, No. 9, pp. e1764–e1768, 2017. DOI: 10.7205/MILMED-D-16-00390
5. W. Sullivan-Kwantes, L. Goodman, The new cold war, Temperature, Vol. 4, No. 4, pp. 341–344, 2017. DOI: 10.1080/23328940.2017.1381799
6. L. Pļaviņa, Is the cold friend or enemy for soldiers in military action?, Rural Environment. Education. Personality, Vol. 16, pp. 29–34, 2023. DOI: 10.22616/REEP.2023.16.003
7. C. Marrao, P. Tikuisis, A. A. Keefe, V. Gil and G. G. Giesbrecht, Physical and cognitive performance during long-term cold weather operations, Aviation, Space and Environmental Medicine, Vol. 76, pp. 744–752, 2005.
8. B. Yan et al., A cold-health watch and warning system applied to the province of Quebec (Canada), Science of the Total Environment, Vol. 741, pp. 140188, 2020. DOI: 10.1016/j.scitotenv.2020.140188
9. S. Hajat, Z. Chalabi, P. Wilkinson, B. Erens, L. Jones and N. Mays, Public health vulnerability to wintertime weather: time-series regression and episode analyses of national mortality and morbidity databases to inform the cold weather plan for England, Public Health, Vol. 137, pp. 26–34, 2016. DOI: 10.1016/j.puhe.2015.12.015
10. T. M. Ikäheimo et al., Cold weather-related cardiorespiratory symptoms predict higher morbidity and mortality, Environmental Research, Vol. 191, pp. 110108, 2020. DOI: 10.1016/j.envres.2020.110108
11. V. Dupade, B. Premachandran, R. S. Rengasamy and P. Talukdar, Survival time of humans in extreme cold climate: Experimental, numerical and parametric study on ambient temperature, fabric insulation and metabolic heat, ASME Journal of Heat and Mass Transfer, Vol. 145, No. 7, pp. 1–31, 2023. DOI: 10.1115/1.4056487
12. T. T. H. Kieu et al., Indigenous knowledge in climate change adaptation: Case studies of ethnic minorities in the northern mountain region of Vietnam, Journal of Vietnamese Environment, Vol. 12, No. 2, pp. 155–161, 2020. DOI: 10.13141/jve.vol12.no2.pp155-161
13. I. Klarzak, E. Ura-Bińczyk, M. Płocińska and M. Jurczyk-Kowalska, Effect of temperature and humidity on heat effect of commercial chemical warmers based on iron powder, Thermal Science and Engineering Progress, Vol. 6, pp. 87–94, 2018. DOI: 10.1016/j.tsep.2018.03.006
14. C. W. Podella, chemical heating pad with differing air-admitting perforation sets for different heat-generation levels, US Patent US4756299A, 1988.
15. E. Irzmańska, M. Jurczyk-Kowalska, Assessment of the thermal effectiveness of mineral warmers for protective gloves used in cold environments, International Journal of Heat and Technology, Vol. 38, No. 1, pp. 28–36, 2020. DOI: 10.18280/ijht.380104
16. P. Schober, C. Boer and L. A. Schwarte, Correlation coefficients: Appropriate use and interpretation, Anesthesia & Analgesia, Vol. 126, No. 5, pp. 1763–1768, 2018. DOI: 10.1213/ANE.0000000000002864
17. X. Xu et al., A digital tool for prevention and management of cold weather injuries - cold weather ensemble decision aid (CoWEDA), International Journal of Biometeorology, Vol. 65, No. 8, pp. 1415–1426, 2021. DOI: 10.1007/s00484-021-02113-0
18. H. A. M. Daanen, Finger cold-induced vasodilation: a review, European Journal of Applied Physiology, Vol. 89, No. 5, pp. 411-426, 2003. DOI: 10.1007/s00421-003-0818-2
19. J. M. Stocks, N. A. Taylor, M. J. Tipton and J. E. Greenleaf, Human physiological responses to cold exposure, Aviation, Space and Environmental Medicine, Vol. 75, No. 5, pp. 444–457, 2004.
20. T. Mäkinen, Human cold exposure, adaptation and performance in a northern climate, International Journal of Circumpolar Health, Vol. 65, No. 4, pp. 369–370, 2006. DOI: 10.3402/ijch.v65i4.18118
21. A. P. Gagge, J. A. J. Stolwijk and J. D. Hardy, Comfort and thermal sensations and associated physiological responses at various ambient temperatures, Environmental Research, Vol. 1, No. 1, pp. 1–20, 1967. DOI: 10.1016/0013-9351(67)90002-3
22. F. S. Bauman, T. G. Carter, A. V. Baughman and E. A. Arens, Field study of the impact of a desktop task/ambient conditioning system in office buildings, Proc. ASHRAE Winter Meeting, San Francisco, CA, 1998, pp. 1153–1171.
23. ASTM C1055-20, Standard guide for heated system surface conditions that produce contact burn injuries, ASTM International, West Conshohocken, PA, 2020.
24. M. D. Langer, W. Huang, A. Ghanem, Y. Guo and G. K. Lewis, Skin temperature increase mediated by wearable, long-duration, low-intensity therapeutic ultrasound, AIP Conference Proceedings, 2017. DOI: 10.1063/1.4977642
25. K. Knecht, N. Bryan-Kinns and K. Shoop, Usability and design of personal wearable and portable devices for thermal comfort in shared work environments, BCS Learning & Development, 2016. DOI: 10.14236/ewic/hci2016.41
26. J. S. Petrofsky, M. Laymon, L. Berk and G. Bains, Effect of thermacare heatwraps and icy hot cream/patches on skin and quadriceps muscle temperature and blood flow, Journal of Chiropractic Medicine, Vol. 15, pp. 9–18, 2016. DOI: 10.1016/j.jcm.2015.12.002